Guideline Highlights:
- Several in-hospital treatments and post-discharge therapies for people who have had an intracerebral hemorrhage, or a bleeding stroke, are not as effective as health care professionals once thought. Compression socks or stockings, anti-seizure medicines and steroid treatment are among treatments with uncertain effectiveness.
- Studies show that minimally invasive surgical procedures may be a useful addition to treating some bleeding strokes.
- People should wait 24 hours after a bleeding stroke to begin rehabilitation activities and functional task training, as mobilization within 24 hours is linked with worse outcomes.
- Home caregivers should receive education, training and practical support to help a stroke survivor’s balance, activity level and overall quality of life.
Embargoed until 4 a.m. CT / 5 a.m. ET Tuesday, May 17, 2022
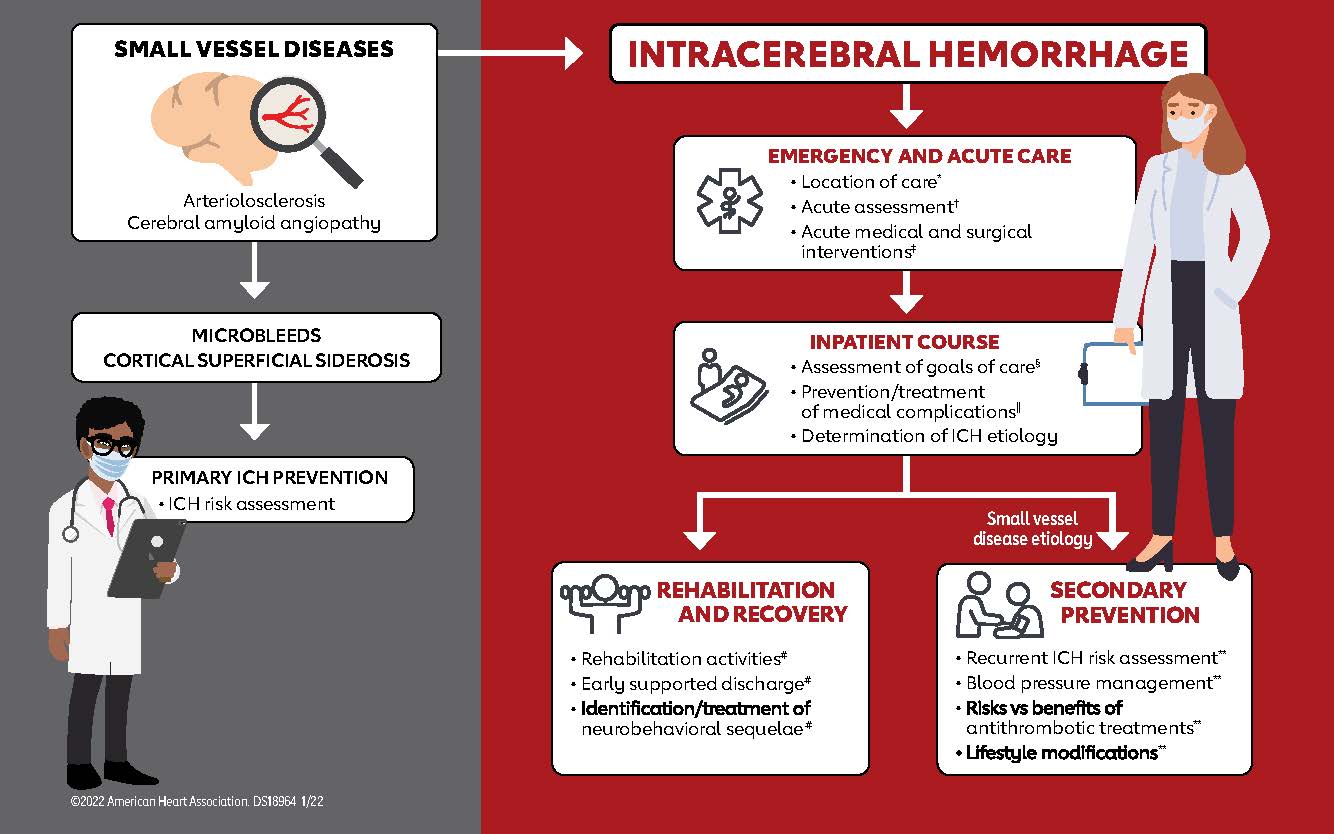
DALLAS, May 17, 2022 — Some treatments or preventive therapies used to manage intracerebral hemorrhages (ICH), or a bleeding stroke, are not as effective as previously believed, according to the new American Heart Association/American Stroke Association guideline for caring for people with spontaneous ICH, published today in the Association’s Stroke journal. Guidelines detail the latest, evidence-based treatment recommendations and are the Association’s official clinical practice recommendations.
The guideline includes recommendations on surgical techniques, individual activity levels after an ICH, and additional education and training for at-home caregivers. It reflects the steady informational gains made in the intracerebral hemorrhage field since the last guideline on ICH management was published in May 2015.
“Advances have been made in an array of fields related to ICH, including the organization of regional health care systems, reversal of the negative effects of blood thinners, minimally invasive surgical procedures and the underlying disease in small blood vessels,” says Steven M. Greenberg, M.D., Ph.D., FAHA, chair of the guideline writing group, a professor of neurology at Harvard Medical School and vice chair of neurology at Massachusetts General Hospital, both in Boston.
ICH accounts for about 10% of the nearly 800,000 strokes that occur annually in the U.S. Typical causes of primary ICH (i.e., ICH not due to another condition such as head trauma) include uncontrolled high blood pressure and age-related degeneration of the brain’s blood vessels. ICH is also one of the deadliest types of strokes, with a 30% to 40% death rate. ICH affects Black and Hispanic people at a rate 1.6 times higher than white people according to U.S. studies. Worldwide, stroke (of any kind) is the second-leading cause of death and a leading cause of long-term disability.
The likelihood of an ICH increases sharply with age, so as the population gets older, these types of strokes are expected to remain a significant health concern. Additionally, the widespread use of blood thinners is a growing cause of ICH. Therefore, new treatments for ICH and improved use of evidence-based approaches are needed for ICH prevention, care and recovery.
Updates to Standard Care Practices
The new guideline suggests that many techniques widely considered “standard care” are not necessary. For example, research confirms that wearing compression socks or stockings of any length to prevent deep vein blood clots, known as deep vein thrombosis, after a bleeding stroke is not effective. Instead, a method known as an intermittent pneumatic compression, which involves wrapping the lower legs and feet in inflatable boots, may be helpful if started on the same day of an ICH diagnosis. Further information is needed, though, on whether using compression stockings in combination with medication may prevent blood clots from developing.
“This is an area where we still have a lot of exploration to do. It is unclear whether even specialized compression devices reduce the risks of deep vein thrombosis or improve the overall health of people with a brain bleed. Even more research is needed on how new blood clot prevention medications may help, especially within the first 24 to 48 hours of the first symptoms,” says Greenberg.
Also updated are recommendations for the use of anti-seizure medicines or anti-depressants after a bleeding stroke. The guideline states that neither of these classes of medications helps a person’s overall health unless a seizure or depression is already present, therefore, they are not advised for most people. Anti-seizure medication did not contribute to improvements in functionality or long-term seizure control, and the use of anti-depressants increased the chance of bone fractures.
The guideline writing group also addresses previously standard in-hospital therapies. They suggest administering steroids to prevent complications from a bleeding stroke is ineffective and highlight that platelet transfusions, unless used during an emergency surgery, may worsen the stroke survivor’s condition.
Surgical Intervention
People with a bleeding stroke may have increased pressure in the brain after the bleed, which can damage brain tissue. These people should be considered candidates for immediate surgical procedures to relieve the pressure, according to the guideline. This is typically done through an opening in the skull to relieve pressure, and in some cases additional techniques may be used to drain excess fluid. The guideline committee reviewed the latest data on minimally invasive surgical techniques, requiring a smaller opening through the skull. Some research suggests procedures with a less invasive approach are less likely to damage brain tissue while removing the fluid build-up.
“The evidence is now reasonably strong that minimally invasive surgery may improve the likelihood that a patient will survive following a moderate or large ICH,” says Greenberg. “It is less clear, however, whether this or any other kind of surgical procedure improves the chances of survival and recovery from ICH, which are our ultimate goals.”
Recovery and Rehabilitation
Stroke rehabilitation includes several strategies to help restore the individual’s quality of life, and the guideline reinforces the importance of having a multi-disciplinary team to develop a plan for recovery. Research suggests a person with a mild or moderate ICH may begin activities like stretching, dressing, bathing and other normal daily tasks 24-48 hours after the stroke to improve survival rate and recovery time; however, moving too much or too intensely within 24 hours is linked to an increased risk of death within 14 days after an ICH.
The guideline outlines several areas for future study, including how soon individuals may return to working, driving and participating in other social engagements. Health care professionals also need more information on recommendations for sexual activity and exercise levels that are safe after a stroke.
Home Caregivers
The guideline recommends education, practical support and training for family members so they may be involved and knowledgeable about what to expect during rehabilitation.
“People need additional help with these lifestyle changes, whether it’s moving around more, curbing their alcohol use or eating healthier foods. This all happens after they leave the hospital, and we need to be sure we are empowering families with the information they may need to be properly supportive,” Greenberg adds.
Education for family or other caregivers benefits the individual’s activity levels and quality of life. Practical support (such as how to walk safely with the patient) and training (such as how to perform certain exercises) are reasonable and may make performing some rehabilitation exercises at home feasible and lead to improvement in patients’ standing balance.
Other Highlights
The writing group recommends the development of regional health care systems able to provide immediate care for bleeding strokes and the capability to quickly transfer people to facilities with neurocritical care and neurosurgical units, if needed. The guideline emphasizes the importance of methods to educate the public, build and maintain organized systems of care and ensure proper training of first responders.
The guideline suggests there may be an opportunity to prevent ICH in some people. The damage to small blood vessels that is associated with ICH may be seen in magnetic resonance imaging (MRI). MRI is not always performed but may be useful for some individuals. In addition, major risk factors for small vessel damage are high blood pressure, Type 2 diabetes and older age. Blood thinners remain an important topic since the use of these medications may increase complications and death from a bleeding stroke. The writing group provides updated guidance for immediate reversal of the newer blood thinners like apixaban, rivaroxaban, edoxaban and dabigatran, as well as older medications like warfarin or heparin.
Renewed emphasis is placed on the complexities of a do-not-attempt-resuscitation (DNAR) status versus the decision to limit other medical and surgical interventions. The writing group highlights the need to educate medical professionals, stroke survivors and/or the individual’s caregiver about the differences. The guideline recommends the severity of a hemorrhage, as measured by the standard scales, not be used as the sole basis for determining life-saving treatments.
“There is no easy path to preventing or curing bleeding strokes, yet there is encouraging progress across all aspects of this disease, from prevention to in-hospital treatment and post-hospital recovery. We believe the wide range of knowledge set forth in the new guideline will translate into meaningful improvements in ICH care,” Greenberg says.
This guideline was prepared by the volunteer writing group on behalf of the American Heart Association/American Stroke Association. Association guidelines detail the latest, evidence-based treatment recommendations and are the Association’s official clinical practice recommendations for various cardiovascular diseases and stroke conditions.
Co-authors are Vice Chair Wendy C. Ziai, M.D., M.P.H., FAHA; Charlotte Cordonnier, M.D., Ph.D.; Dar Dowlatshahi, M.D., Ph.D., FAHA; Brandon Francis, M.D., M.P.H.; Joshua N. Goldstein, M.D., Ph.D., FAHA; J. Claude Hemphill III, M.D., M.A.S., FAHA; Ronda Johnson, M.B.A.; Kiffon M. Keigher, D.N.P., A.C.N.P.-B.C., R.N.; William J. Mack, M.D., M.S., FAHA; J. Mocco, M.D., M.S., FAHA; Eileena J. Newton, M.D.; Ilana M. Ruff, M.D.; Lauren H. Sansing, M.D., M.S., FAHA; Sam Schulman, M.D., Ph.D.; Magdy H. Selim, M.D., Ph.D, FAHA; Kevin N. Sheth, M.D., FAHA; Nikola Sprigg, M.D.; and Katharina Sunnerhagen, M.D., Ph.D. Authors’ disclosures are listed in the manuscript.
The Association receives funding primarily from individuals. Foundations and corporations (including pharmaceutical, device manufacturers and other companies) also make donations and fund specific Association programs and events. The Association has strict policies to prevent these relationships from influencing the science content. Revenues from pharmaceutical and biotech companies, device manufacturers and health insurance providers and the Association’s overall financial information are available here.
Additional Resources:
About the American Heart Association
The American Heart Association is a relentless force for a world of longer, healthier lives. We are dedicated to ensuring equitable health in all communities. Through collaboration with numerous organizations, and powered by millions of volunteers, we fund innovative research, advocate for the public’s health and share lifesaving resources. The Dallas-based organization has been a leading source of health information for nearly a century. Connect with us on heart.org, Facebook, Twitter or by calling 1-800-AHA-USA1.
###
For Media Inquiries: 214-706-1173
Maggie Francis: 214-706-1382; Maggie.Francis@heart.org
For Public Inquiries: 1-800-AHA-USA1 (242-8721)
heart.org and stroke.org





Leave a Reply